

Introduction and Overview
Discussions on healthcare in Canada typically revolve around spending and who pays. The people’s actual needs for healthcare and support get less attention and even less action. Yet far too many Canadians lack access to timely primary care and experience long wait times for services; planning is inadequate for the surging needs of the population of older seniors and, among other issues, the fundamental one of optimizing population health, or addressing mental health and addiction, have never received adequate attention. Like the myth of Sisyphus, many attempts, most based on cost-saving objectives, have been made to push fundamental change in the governance, management, structure, function, and accountability of health services in Canada. Why do they continue to be unsuccessful? What are the roadblocks and how might they be overcome? This Roadmap addresses these questions in its design of a more effective reform process. Its recommendations reflect the input of 23 expert reviewers and a review of this literature represents a general consensus on viable options ahead.
Perhaps the most formidable roadblock has been public tolerance of the status quo originating in the once iconic reputation of Canada’s publicly funded healthcare and fear that change with its usual cost-saving objective will bring us closer to how our southern neighbours do healthcare – higher costs, poorer outcomes, and relative exclusion of the poorer and under-insured of their citizens. Even discussing change to medicare has been said to be the equivalent of grasping the electrified third rail. How might such tolerance and fear be overcome, replaced with confidence that fundamental change in Canada’s health services “system” can make it more effective, efficient, productive and affordable, and change more comforting than frightening?
The timing is right. With the lingering effects of the COVID pandemic and especially the now widespread frustrations Canadians have in accessing primary care and with long wait times for many health services, including emergencies, people’s one-time confidence in their publicly funded (perceived to be free) health services is badly shaken. Politicians ignore this public sentiment to their peril. They should seize the opportunity to engage the public and health service providers to address these concerns. While recent federal and provincial governments initiatives are welcome, such as to increase staffing levels, a much more holistic and comprehensive reform agenda is required. That is the focus of this Roadmap. Implementing its recommendations should yield cost savings, but service improvements are its primary focus. In that vein, this paper also briefly highlights, in separate sidebars, signs of progress on the healthcare file in different jurisdictions.
Some previous reform efforts have hit the shoals because the required foundations such as better information and human resource planning were not in place. When supplemented by the good, more inclusive and timely data recommended by the Roadmap together with comprehensive measures of the health of Canadians relative to others in the developed world, a compelling case for reform can readily be made. Health services are labour-intensive, yet until recently scant attention has been paid to the need for workers and how those needs would change under reform. This Roadmap recommends a structure for human resource planning.
The siloed leadership structure of the health sector has plagued previous reform initiatives. Change has usually been directed centrally, typically by a provincial ministry of health, without adequate input from the regional and local health authorities charged with service delivery. The resistance has been magnified by siloed budgeting, giving little or no opportunity for those authorities to organize funding to best meet needs. This Roadmap addresses both governance and funding structures. We are a democracy. Let the people affected govern, more closely manage, and take much more responsibility for the effectiveness of the health system that serves them; take it out of the hands of far-away government bureaucrats.
Previous reform initiatives have often been but partial in scope. Yet all parts of the health sector must function together smoothly; one cannot typically be improved without supportive changes being made elsewhere. For example, the oft-recommended re-jigging of “scopes of practice,” whereby professionals focus on where they have a comparative advantage, cannot work effectively under siloed budgets. The Roadmap offers a holistic plan in which those interrelationships are recognized, pairing changes that need to go together, and sequencing according to priority.
Overcoming resistance to changes in health with well-informed opinion of the status quo is not the only way around the roadblocks. Doing that though is important politically to spur our provincial, territorial, and federal governments to work closely together and also get them to recruit to their discussions municipal governments with their heavy sway over health’s powerful social determinants. The goal: to enable Canadians to be among the healthiest in the world.
Investing in the fast-developing new technologies of Artificial Intelligence and Machine Learning offers the opportunity to change the now frightening imbalance between the provision of health services and the administrative/record-keeping chores that consume so much of the care and support-giving time and expertise of doctors, nurses, therapists, and other health professionals. Development of a Canada-wide Clinical Information System, while expensive at the front end, would pay a substantial dividend in eliminating duplicated and difficult-to-share- information, even with the patients who are their health record’s prime beneficiaries. Important as it is to “buy change”, saving the taxpayers’ and private payers’ money today is secondary in the current environment to ensuring health services’ affordability down the road. This is due to the imperatives of reducing Canada’s pre-existing debt burden, limiting and adapting to climate change, population ageing, and other long-deferred and poorly financed imperatives like public housing, financial and personal security, and others of the social determinants of health.
Canada’s young health professionals are increasingly unwilling to be simultaneously business-owners and providers of the health services for which they are trained. Fostering their working collaboratively in multidisciplinary teams relieved of business responsibilities and assured of employee benefits would go a long way to attract and retain them in primary care, nursing, counselling, social work, and personal support – health worker fields increasingly difficult to fill. The scopes of practice of many if not all health providers need to be adjusted given now applicable educational and experiential standards; who better to undertake the changes but the leaders of the team-based health professions themselves working together? The challenges and wisdom of potential scope of practice “fixes” are well known to them.
All of this and more will be hard to do, together with getting a handle on foundational up-to-date and timely data-record and clinical information systems. But the longer we delay the harder change will be, and the unhappier people will be with health services in Canada. The time is over-ripe to forge a consensus, rally around an agreed plan of reform and get on with its implementation!
In this Roadmap we summarize those elements of known reform proposals we believe hold promise, including especially their potential for mutual reinforcement, grouped under foundational support, priorities to be implemented now, actions with longer horizons, and proposals that have yet to find broad consensus.
The times are changing. The growing angst of Canadians makes reform a viable option now, if the focus is squarely aimed on delivering what Canadians want. Roadmap sets out a plan to take us to the twin destination of better health for more Canadians and secure and readier access to high-quality healthcare.
This paper develops a presentation by Don Drummond to the C.D. Howe Institute’s Health Policy Council on May 31, 2023.
The roadmap for reforms in this paper reflects the input of expert reviewers. We thank Owen Adams, Bob Bell, Janet Davidson, William Falk, Vivek Goel, Simon Hagens, Mike Hamilton, Health Canada, Zayna Khayat, Alika Lafontaine, Shoo Lee, Steven Lewis, David O’Toole, Ito Peng, David Pichora, James Radner, Danyaal Raza, Mark Rochon, Rosalie Wyonch, Katherine Zagrodney and several anonymous reviewers for helpful comments on earlier drafts.
A. Foundational Support
1. Better Data Collection, Analysis, and Reporting
The first step to solving any problem is to understand its nature and source(s) from complete, accurate, and up-to-date information. High-quality data needed for that first step are not available to federal, provincial, territorial and municipal governments. Reform is required to address the needs of patients and to support planning, accountability, performance evaluation and measurement of health outcomes. Federal, provincial and territorial efforts to date should be extended to include steps such as:
- greater consistency/standardization under a federated approach to provincial-territorial health data;
- consistency with accepted international standards;
- rapid expansion and use of fast-advancing technologies (including AI) in its collection, utilization and sharing;
- development of a primary care data set that includes attachment and access information and outcomes measured in terms that matter to people and the costs of achieving them;
- accurate wait times for all referrals and interventions developed through mandatory utilization of e-referrals and e-consults (such information would also be useful for identifying service and workforce gaps);
- complete, timely and standardized data on the supply of and demand for the sector’s workforce;
- measures of health outcomes and population health status;
- measures of advanced performance and prediction analytics;
- increased linkage of aggregated Canadian Institute for Health Information (CIHI) and Statistics Canada data to other sources, including of socio-economic information; and
- greater and timelier central capacity for data analysis and reporting to governments, the “system’s” operators (Integrated Health Systems and Teams for example), health professional and provider organizations, and especially the Canadian public who, as patients, should have access to their own health data.
These proposals have been under discussion for years by those responsible for health data collection, analysis, and reporting. The details of their implementation can be worked out expeditiously by federal-provincial-territorial officials with CIHI as Secretariat.
The federal government should provide the required funding through bilateral agreements with the provincial and territorial governments. The work must not be distracted by suspect links to accountability measures. A start was made with the announcement in the 2023 federal budget of $505 million over five years, starting in 2023-24, for CIHI, Canada Health Infoway, and other federal data partners to work with provinces and territories.
The scale of the data reform challenge is significant in Canada and elsewhere. But it must be met and quickly; all else depends on it!
https://www.canhealth.com/2022/06/01/alberta-expands-connect-care-in-edmonton-calgary/
https://www.cbc.ca/news/canada/edmonton/alberta-health-services-connect-care-pandemic-delays-1.6633054
Long lead times in the education and training of many health providers make clear how essential long-range planning is to meet future labour requirements in the health sector. Here the work should be done under the direction of provincial,-territorial and federal deputy ministers, their officials, and the leaders and educators of the health professions.
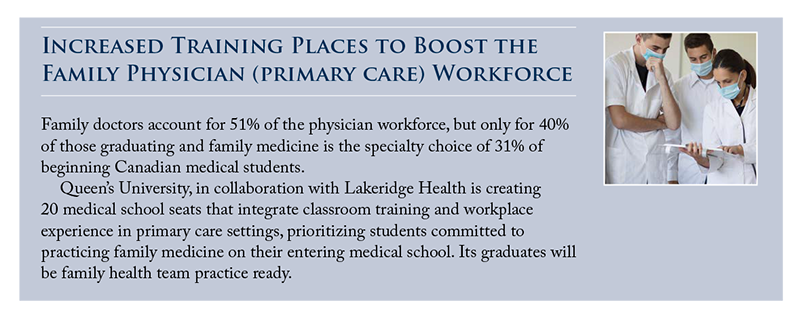
The need for such planning is acute. The example of family physicians illustrates the wide breadth and synergies of the reforms required. The dwindling proportion of Canadian-trained medical students and graduates choosing to specialize as family physicians, once half, makes clear that without actions being taken soon the access problems to primary care, now bad, will only get worse.
Some responsibilities can be shifted from family physicians by expanding the scopes of practice of nurse practitioners, nurses, pharmacists and others but many of these, too, are in short supply and relatively few are being trained in relation to the demand. Health human-resource planning must not be rigid but recognize the potential for changed roles of healthcare workers and the technological changes that will also have profound impacts on their numbers, qualifications, and competencies.
Training and work assignments in healthcare are typically oriented around credentials. Greater attention to competencies, which might be a sub-set of what is covered under credentialing, could be a strategic way to address shortages of workers in specific areas through mini-training courses and work specialization in areas of high demand.
Increasing the supply and retention of Personal Support Workers (PSWs) and other community workers in support of the elderly’s ageing well is also urgently required. This will require, among other things, improved conditions of work and efforts to elevate the status of the occupation.
Little is known about the balance, either currently or in the long term, between the supply and demand for physiotherapists, pharmacists and other health professions and practitioners. That too must be rectified despite the challenge that many allied health fields lie outside Canada’s publicly insured “system.”
Finally, many in the healthcare workforce are burned out from COVID 19 and other pressures. Healthcare’s providers must ensure that sustainable work practices are implemented to support workers’ well-being and particularly their retention in their fields of support and care.
1) https://www.immigration.ca/ontario-plans-foreign-trained-doctor-credential-recognition-program/
2) https://www.cbc.ca/news/canada/toronto/ont-international-nurses-1.6535290
 https://www.cdhowe.org/sites/default/files/2022-11/Commentary%20630.pdf
https://www.cdhowe.org/sites/default/files/2022-11/Commentary%20630.pdf
 https://www.health.gov.au/our-work/national-medical-workforce-strategy-2021-2031
https://www.health.gov.au/our-work/national-medical-workforce-strategy-2021-2031
B. Priority Reforms that Should Be Implemented Now
These reforms can be implemented now and would mutually support the preceding foundational steps on information and human resource planning.
3. Team-based Health Service Models
Team-based practices began decades ago with Health Maintenance Organizations that morphed into many forms, operating under a variety of names encompassed by the general description of Integrated Health Systems (IHSs). In Canada, teams of care were pushed in the early 2000s, waned for a while but are waxing again, driven by the growing preference of young physicians for team and employment-model practices, coupled with recognition by governments that previous attempts to manage their systems with one-size-fits-all policy have failed. Yet only three provinces, Alberta, Ontario and Quebec foster significant use of primary care teams; even there, teams should be more strongly promoted. Newfoundland and Labrador and British Columbia have been increasing the number of teams in primary care.
In some provinces and territories, centralization is being replaced by plans to devolve leadership and operational responsibility for health services to regional teams of providers and representatives of the populations they serve. Nova Scotia and Ontario in particular, are making steps in this direction. Such teams need to ensure that all members are working at their “full scope.”
Primary care teams should be responsible not only for their rostered clients, but also for those of adjacent neighbourhoods. By doing so, a population health approach would shape the organization of primary care.
Objectives and data must be carefully calibrated in any drive toward more team-based practices. The Ontario Government froze new family health teams out of concern they were not producing the outcomes desired, but analysis of their performance was made difficult because neither the objectives nor the performance data to measure them were clearly specified.
In some cases – care and rehabilitation of addictions and mental health being an example – teams must be quite broad in scope. Health Teams, which are natural central hubs, need partnerships with municipalities, community and social services and government ministries involved both with the support of health’s social determinants as well as that of healthcare services.
A few key features to be achieved through teams include the following.
- accountability agreements that begin with universal enrolment (i.e., the entire population has access to a team).
- accountability agreements linked to service provision and to the extent possible, health outcomes.
- patients, families and communities being part of the team.
- after-hours access to primary care built into the accountability agreements.
- extended service hours for lab and imaging diagnostics with the results available outside of hospitals to assist in primary care decisions made after hours.
- reduction of the substantial administrative burden on family physicians and teams through means including Artificial Intelligence, scribes, form standardization, and elimination of work accomplishing little (see a box referencing the initiative to reduce administrative burden in Nova Scotia).
- exploration of alternative structures that might include the private sector, provincial governments or municipalities to build clinics in which teams would work, reflecting the growing preference of young physicians to focus on practicing medicine as opposed to running a business and owning real estate.
- as discussed below, with the involvement of Primary Care Councils, carefully expand the use of care plans, e-consults, and common intake specialty consultation processes.
- implementation of scopes of practice as appropriate.
- reform of funding and pay provisions to support the recommended reform of primary care.
Note that many of these elements would relieve pressure on hospitals and Emergency Departments in particular.
4. Expanding Scopes of Practice
There is great promise in re-examining the scopes of practice of several, if not all, the health professions that current high admission and educational standards render antediluvian. Their resetting could well relieve stresses from the lack of ready availability of some providers, as nurse practitioners and others are now doing in primary care. With so few geriatricians and other specialists dealing with the needs of seniors, yet more pressure will fall on family physicians and nurse practitioners already in short supply.
An oft-cited example of a change in scopes of practice is nurse practitioners performing more functions typically done by physicians. This could also involve organizational change whereby nurse practitioners work independently from physicians more often. Licensed practical nurses could assume many functions currently performed by registered nurses. Many more examples could be given.
https://www.saskatchewan.ca/government/news-and-media/2022/june/23/rapi… (June 2022)
https://news.gov.bc.ca/releases/2022HLTH0212-001619
https://nationalpost.com/news/canada/cp-newsalert-b-c-government-offers-new-pay-model-for-doctors-to-help-health-crisis
https://news.ontario.ca/en/release/1002633/pharmacists-now-treating-thirteen-common-ailments-and-renewing-prescriptions-for-most-medications
https://doctorsns.com/contract-and-support/admin-burden
Widening scopes of practice is not risk free. High quality patient care must prevail, and false economies avoided. Nevertheless, this reform offers considerable promise.
5. Changed Models of Professional Recompense and Institutional Funding
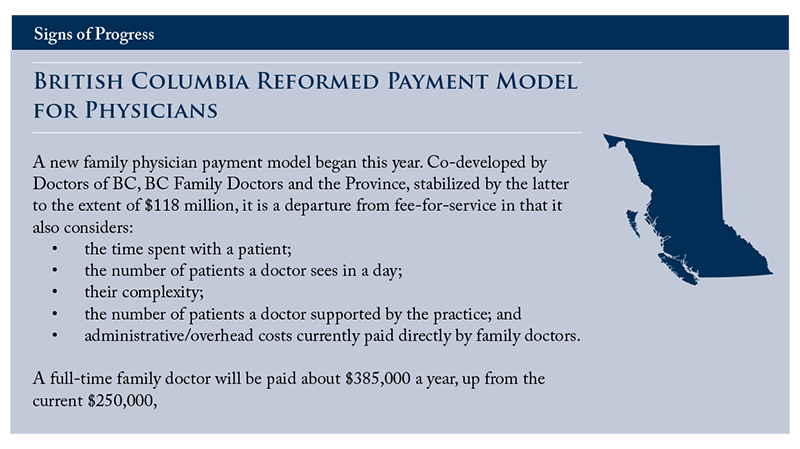
Declining slowly, fee-for-service remains the dominant form of physician compensation, a form that can lead to “over-servicing” just as fixed incomes can lead to “under-servicing.” Growing is a preference for fixed payments/capitation models but combined with quantitative and qualitative measures of health outcomes and patient satisfaction. It is likely that compensation models for primary care should maintain their emphasis on patient access. The government of Newfoundland and Labrador recently reached an agreement with the Medical Association on a new Blended Capitation Payment Model for family physicians that pays doctors a set annual fee for each attached patient, plus a reduced fee-for-service each time they see that patient.
With respect to their funding, neither global fixed budgets for hospitals nor activity-based funding is perfect. The United Kingdom provides a useful case study. Activity-based funding led over time to the introduction of thousands of additional codes that increased administrative work and costs. Recently the National Health Service (NHS) moved back to a ‘blended payment’ approach,
For Canada, some comparable “middle way” offers the best opportunity. Any changes should be also made gradually, especially now as all “system” participants still struggle with the sequelae of the COVID pandemic.
Activity-based funding should be adopted for all interventional procedures. Bundled payment is useful for interventions by teams that may span organizational boundaries.
6. Regional Health Bodies with Global Budgets
The needs of the varied population in any area are difficult to meet through centralized health governance. A preferred structure is a regional health body with a global budget within which the governing body can adjust services and funding to meet best its population’s needs. A regional governance structure would facilitate the use of health teams, expanded scopes of practice and optimal use of facilities and personnel. It could also better blend supports such as healthcare, education and social services to optimize population health. On paper, some regional structures, such as Ontario Health Teams, appear to have the structure recommended, but in practice to date they have neither the authority nor the resources to govern or manage services within their region. Some provincial approaches to regionalization address specific services only, such as Quebec’s PREMs which distribute medical staff geographically based on the gaps between the workforce in place and the needs in each region.
Regionalization must be more than a geographical concept. Clear roles, responsibilities and accountabilities of the regional authorities must be enunciated. The central government authorities must also have their clearly enunciated roles and responsibilities. Resources in amount and discretion in use must align with the roles and responsibilities. Care must be taken to avoid duplication and particularly where accountability falls for the outcomes of decision-making.
Without diminishing in the least the importance of any others, the priority given the preceding six reforms to be undertaken right away have been selected primarily with respect to:
- the urgency of their being implemented as stepping stones to achieving overall health system reform; and
- their do-ability and progress already made.
C. Reforms with Longer Horizons
7. Redefining Long-Term Care to Encompass a Continuum Including Homecare and Community- Based Living
The initials LTC have become a synonym for institutional nursing homes. It ignores that fact that most elderly people strongly prefer to, and do, age well in their own homes and communities or environments like them. To do so safely and well they require services more in the nature of support for their daily living than care per se. That Canada’s population 75+ in age will double over the next 20 years and significantly increase the need for such services is a fact long known but yet to be acted upon by all governments. The latter include the one that stated, “helping Canadians age with dignity, closer to home, with access to home care or care in a safe long-term care facility is another area of priority.”
https://venturebeat.com/healthtech/digital-innovation-across-the-patient-journey-for-kaiser-permanente/
https://venturebeat.com/data-infrastructure/kaiser-permanente-cdo-on-health-care-digital-transformation/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10050950/
This will require more funding, including for additional institutional capacity, potentially extending access all the way to universal coverage. Health Ontario, for example, has committed to creating 30,000 new long-term care beds by 2028; that target should be expanded to include, as a LTC policy objective, home and community care as well as beds. Hand-in-hand with greater capacity, is more full-time employment and improved working conditions for PSWs, nurses and other support workers.
To repeat, expanding home and community care appears a very promising reform, offering better patient outcomes, satisfaction, cost-effectiveness, and reduced wait lists for facility-based care. It would also dovetail with improvements in remote monitoring, data and digital access, and facilitating more effective virtual care.
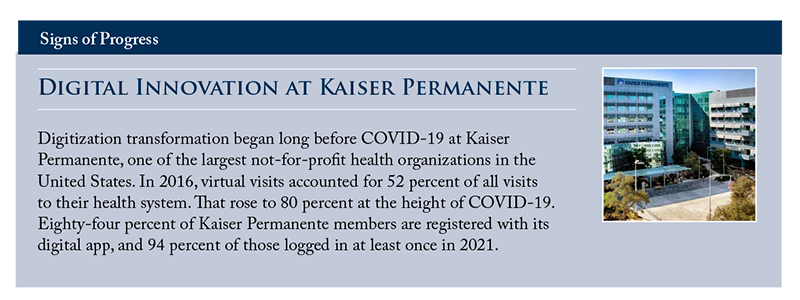
8. Digital Health Services and Solutions Transformation
Providing services digitally, of which remote care is a sub-set, is clearly efficacious in rural and remote areas where no alternatives are available. It may also be beneficial in urban areas with difficult primary care access. Until the population’s timely access to face-to-face primary care is improved, it is highly likely that access via digital/electronic links will remain a valuable addition to the technical armamentarium of the providers of primary care and others, social and other community workers for example. Virtual care offers the opportunity for improving equity of care by improving access for the populations currently the most under-serviced. It also offers scope for potential further innovation such as integration into electronic medical records of information from personal “wearable tech.” But such services should not just be allowed to “happen.” They should be planned carefully based on the availability of the results achieved through insightful research. Let’s not let the cart get ahead of the horse! The destination is likely a hybrid physical-virtual care model.
A better way must be found to spread and scale innovation in healthcare generally. It is often lamented there is not a “national” healthcare system, but its fragmentation across geography does facilitate experimentation. Where the experiments are successful, they need to be spread and scaled up. That requires effective information dissemination, a challenge within health’s current governance structure. Healthcare Excellence Canada performs the role to a degree. The 2015 Advisory Panel on Healthcare Innovation recommended going further and called for the federal government to invest in an arm’s-length healthcare innovation fund that would finance initiatives, break down structural barriers and accelerate promising innovations. The case remains valid but has not been implemented.
9. Scopes of Sites of Healthcare
A primary reason for over-crowding in Emergency Departments (ED) is hospital beds being occupied by patients awaiting long-term care placement to more appropriate sites of care. Patients in the ED requiring admission therefore wait hours for an in-patient bed, creating overload in the ED. Addressing the needs of these people, typically elderly, through home care, community-based living and long-term facilities, would ease the capacity pressures on hospitals. As would expanded access to out of hours primary care in clinics and other sites outside hospitals. ED throughput could be sped up by greater investment in less acute, rehabilitation-focused transitional-care facilities to provide more effective support and care for recovering hospital patients and free up acute beds. Recently established models of virtual emergency primary care can triage and reduce unnecessary ED visits.
For pre-planned, elective care, dedicated out-of-hospital for- and not-for profit surgical and diagnostic centres could reduce backlogs.
Both are critical areas to address, but top priority should go to enhancing people’s access to primary care, the preferred entry point to the “system”. Among the many ‘flash points’ are those families, including children, once well served, whose family doctor has retired and whose potential successor practitioners are reluctant or unwilling to accept them on their rosters.
10. Improved Accessibility to Reduce Health Inequalities
Rural, Indigenous and racialized communities typically have inconsistent access to healthcare and poor health outcomes. Rural areas have approximately 18 percent of the Canadian population but 8 percent of physicians,
Expanding virtual care is a promising reform initiative that can tap into federal, provincial and territorial efforts to broaden access to high speed internet. A recent innovation in Ontario includes a provincial emergency department peer-to-peer program to provide additional on-demand, real-time support and coaching from urban emergency physicians to aid attending family physicians in rural EDs. But the local workforce and its scopes of practice must also be enhanced.
Finally, action is needed to address inequalities in the social determinants of health, including housing and employment, especially in Canada’s Indigenous communities.
11. Greater Emphasis on Health Promotion and the Avoidance of Ill-health
Good health is an outcome of both health’s promotion and healthcare. The treatment of ill-health and the restoration of good, has been the predominant focus of Canada’s health system from its inception. In contrast, the broader (and more impactful) social determinants of health (housing and income, for example) have not claimed anything like equal priority. More “upstream” policies are needed to improve them. The same bias applies to what we measure, procedures and interventional activities to the neglect of their outcomes. Overall, despite the work of the Romanow report (2002) over two decades ago, significant opportunities continue to be missed in relation to improving the population’s health and wellbeing and controlling the system’s ever-growing costs.
Healthcare’s professionals, providers, communities, and government departments alike should support working more closely together in teams to deliver more people-centred support and care. This includes strengthening the essential partnerships between health and social services and, within governments, of cross-ministry and inter-governmental reviews of services, policies, regulations to improve their governance and integration.
A shift to focusing on health outcomes will eventually require the evolution of funding and payment models to re-focus on the system’s results rather than its activities. This could include modifying activity-based payments with respect to specified outcome metrics such as feedback on patients’ experience, as is already the case with US Medicare, the data derived from the soon to be ubiquitous digital wearables, and/or funding based on bundles of support and care to incentivise collaboration and integrated care among multiple health service providers.
Overall, making improvement in this area is challenging. It involves targeting outcomes that we cannot always measure precisely. It involves creating complex teams of professional and institutional providers long used to working independently of others and the implementation of new governance and management arrangements, changes usually unsettling and unwelcome but essential. It also requires the political determination to invest in upstream activities that will provide cost-effective population health improvements but demonstrate benefits only over time. As noted above, improving the data is likely the best place to start. Greater transparency will undoubtedly facilitate and catalyse more and faster reform to create a more real and better system to optimize the health of Canada’s population. It is time to get to it!
D. Proposals Yet to Find Broad Consensus
One of the most controversial topics in Canada’s universal healthcare system is the suggestion that patients pay user fees or co-payments privately in addition to funding derived from taxation for medically necessary care. Despite the principle’s having been abrogated for many years with respect to prescribed medicines, rehabilitation therapy, some diagnostic, non-psychiatric and other equally medically necessary services, recent government announcements make clear how unlikely it is any private-pay options will be seriously considered. Nevertheless, discussion of the topic will continue.
While governments are publicly opposed to private funding models, recent surveys reveal mixed public opinion.
Much attention has been attracted of late to the possibility of opening more facilities like private surgical clinics. We should also be mindful that existing public facilities are not always used to their full potential. Lengthening the working hours of operating theatres, for example, would help ease what is typically described as capacity pressure.
Any debate on co-payments should distinguish whether the purpose is to raise funds or to influence behaviour. Charges aimed at incentivizing people toward more appropriate forms of care, when such options are available, may be more readily accepted by Canadians.
Australia and the United Kingdom provide precedents for public and private systems to operate in parallel, the latter offering a modest release of pressure from rising demand in the public system. Nevertheless, wait times remain problematic there also.
Increased LTC funding could come from an LTC insurance model, like Canada and Quebec Pension Plans; user charges might also be required. Several countries encourage independent living by subsidizing family caregivers. It has also been suggested there be flexibility such that those qualifying for long-term institutional care have the option of augmenting from their own resources services provided by the institution. Some shorter-term options are available to help people fund their care needs in the later years such as deferring the age at which Registered Retirement Savings Funds must begin to be drawn down.
Publicly insured services delivered by private organizations have received considerable attention of late, with the discussion typically focused on whether to grow this model to address capacity issues in the public sector. Information is again key. There must be valid comparisons of benefits and costs in public and private delivery options.
13. Broadening the Coverage of Universal Healthcare
The inclusivity in Canada of universal health coverage continues to be debated. The most recent areas for debate are pharmaceutical, dental, and mental health and addictions care. The federal government has identified some funding to help provinces and territories expand mental health coverage. The 2023 federal budget announced that by 2025, the Canadian Dental Care Plan will be fully implemented to cover all uninsured Canadians with an annual family income under $90,000. The coverage is to be provided without any co-payments.
The situation is the product of the system’s history and evolution. Clearly the cost of increasing the scope of universal coverage is a significant barrier to change, although to a large extent the cost would not be increased but rather transferred from out-of-pocket private payments to public funding. There are significant but rarely acknowledged gaps now in coverage for services that are already theoretically covered by the Canada Health Act, medically prescribed drugs, for but one example. Further expansion of universal coverage should identify sources of funds rather than implicitly adding to borrowing and passing the burden to future generations.
Alternatives to expanding universal coverage have been proposed. Ontario is examining a portable health benefit to follow workers as they move from job to job and cover workers in jobs without benefits, including self-employment, contracting, part-time, and temporary or gig-type jobs. The C.D. Howe Institute recommends an expansion of the medical expenses tax credit to better enable people to meet their non-insured health needs.
Conclusion
All these policy issues have been discussed in many fora over the past sixty years and more, with action on implementing the resultant recommendations being “kicked down the road” to be dealt with later by other governments, bureaucrats, hospitals and other institutional providers and health professionals. It’s now later and has been for quite a while!
References
Ahmed, H., and I. Bourgeault. 2022. Sustaining Nursing in Canada, CHWN, CFNU. 2022
Blomqvist, Ake. 2022. The Dutch Model: A Cure for What Ails Canadian Healthcare? Commentary. Toronto: C.D. Howe Institute. April 2022
Allin, S., et al. 2022. Sustainability and Resilience in the Canadian Health System: A PHSSR Report, Institute for Health Economics. November.
Armstrong, P. 2021 Our Values Are Showing: Long-Term Care and the Pandemic. CJNL 35 (4). September.
Armstrong P., H. Armstrong and I. Bourgeault. 2022. Teaming up for long-term care: Recognizing all long-term care staff contribute to quality care, Healthcare management forum / Canadian College of Health Service Executives. September.
Association of Municipalities of Ontario. 2022. Strengthening Public Health in Ontario: Now and for the Future, Submission to the Ministry of Health, August.
Bell, R., A. Golden, P. Alofs, and L. Robins. 2022. Canada’s specialist referral system needs to be boosted into the 21st century. Globe and Mail OpEd. May.
___________. 2022. Months-long surgery wait times are the norm in Canada. Dedicated community surgery centres will reduce the backlog, Globe and Mail OpEd. May.
___________. 2022. Nearly 15 per cent of Canadians don’t have a family doctor, but the solution isn’t hiring more, Globe and Mail OpEd. May.
___________. 2022. Personal support workers Personal support workers are critical to caring for Canada’s aging population. Governments need to treat their jobs as essential, Globe and Mail OpEd. May
___________. 2022. The pandemic revealed brutal realities about long-term care. Canada has a moral obligation to fix the system, Globe and Mail OpEd. May.
___________. 2022. Transitional-care facilities will stop Canada’s ERs from resorting to ‘hallway medicine’, Globe and Mail OpEd. May.
Canadian Health Workforce Network. 2022. Submission to House of Commons Standing Committee on Health on Canada’s Health Workforce, March.
Canadian Dental association. 2022. Submission to House of Commons Standing Committee on Health on Canada’s Health Workforce, April.
Canadian Federation of Nurses Unions. 2022. Submission to House of Commons Standing Committee on Health; Study of Canada’s Health Workforce; A Pan-Canadian Framework for Quality Care, March.
Cheff, R., and S. Um. 2021. A new normal for health coverage, Wellesley Institute. November.
CIHR Institute of Population and Public Health. 2022. Moving Forward from the COVID-19 Pandemic: 10 Opportunities for Strengthening Canada’s Public Health Systems, March.
CMA. 2022. Health care funding in Canada, October.
_____. 2022. Recommendations for federal action to address Canada’s health care crisis, Submission to the House of Commons Standing Committee on Finance. February.
CMA, CNA, CFPC. 2022. Joint Submission to the House of Commons Standing Committee on Health (HESA), April.
CNA. 2022. Stop The Bleeding In Canada’s Health Workforce: Recommendations For The Federal Government.
Commonwealth Fund 2021. Mirror, Mirror, 2021: Reflecting Poorly, August.
Cooper D. 2022. Nurse Practitioners’ Association of Ontario, Interview: Advocates call for more nurse practitioner led clinics in Ontario, November.
Drummond, D., and D. Sinclair. 2022. Fixing, Funding, and Reforming Health Services. Toronto: C.D. Howe Institute.March.
Drummond, Sinclair, Queens University, Ageing well, November 2020
Drummond, D., D. Sinclair, and J. Gratton. 2022., Troubles in Canada’s Health Workforce: The Why, the Where, and the Way Out of Shortages, Commentary. Toronto: C.D. Howe Institute. November.
Drummond, D., D. Sinclair, and P. Gladkov. 2021. Best in Health: Creating a Comprehensive Health Information Ecosystem. Working Paper. Toronto: C.D. Howe Institute. August.
Falk, W., and T. Jamieson. 2023. A National Digital Health Architecture is Long Overdue: Let’s Get Going, Toronto: C.D. Howe Institute. May.
Fraser Institute. 2021. Less Ottawa, More Province, 2021: How Decentralized Federalism is Key to Health Care Reform, October.
____________. 2021., Understanding Universal Health Care Reform Options: Activity-Based Funding, June.
___________. 2022. Understanding Universal Health Care Reform Options: Cost-Sharing for Patients, July.
Government of Canada, Health Canada. 2023. Working together to improve health care for Canadians, February 07.
Government of Ontario, Family health teams, April 2022
Government of Ontario. 2022. News release: Local Pharmacies Now a One-Stop-Shop for Thirteen Common Ailments, December.
Government of Ontario. 2023. Your Health: A Plan for Connected and Convenient Care, February.
Government of Ontario, Ministry of Health / Ministry of Long-Term Care. 2019. Hallway Health Care: A System Under Strain. First Interim Report from the Premier’s Council on Improving Healthcare and Ending Hallway Medicine, January.
Health Charities Coalition of Canada. 2021. Mandate Letter for All Parliamentarians, November.
Hunsley, The Pearson Centre. 2022. Are Nurse Practitioners the Solution for Seniors’ Primary Care? April.
Longwoods. 2020. Improving value in healthcare: No silver bullet, Healthcare Papers.
_________. 2020b. The Search for Improving Value in Canadian Healthcare: Holy Grail or Steady Progress, Healthcare Papers.
Marchildon, G., S. Allin, and S. Merkur. 2020 The North American Observatory on Health Systems and Policies (NAO) and The European Observatory on Health Systems and Policies, Health Systems in Transition Canada Health system review 22 (3).
McGrail, K., F. Clement, and M. Law, CIHR Institute for Health Services and Policy Research. 2022. The Value of and Need for Health Services and Policy Research that Focuses on Macro System-Level Challenges, April.
Montgomery, C. J. Sproule, J. Round, and C. McCabe. 2022. Adapting the WHO Best Buys Principles to Frailty Care in Canada, Institute for Health Economics, July.
National Collaborating Centre for Indigenous Health. 2020. Supporting Indigenous self-determination in health: Lessons learned from a review of best practices in health governance in Canada and Internationally, 2020.
NHS England. 2020. 2020/21 National Tariff Payment System, Guidance on blended payments, November.
Ontario Health. 2022. Annual business plan 22/23, May.
_____________. 2022. Plan to Stay Open: Stability and Recovery (5 point plan), August.
Ontario Medical Association. 2021. Prescription for Ontario: Doctors’ 5-Point Plan for Better Health Care, October.
Ontario Nurses Association. 2022. Submission on 2022 Pre-Budget Consultations to Standing Committee on Finance and Economic Affairs, January.
Ontario Premier’s Council on Improving Healthcare and Ending Hallway Medicine. 2019. A System Under Strain: First Interim Report.
Ontario Premier’s council on Improving Healthcare and Ending Hallway Medicine. 2019. A Healthy Ontario: Building a Sustainable Health Care System, 2nd Report, June.
Pan-Canadian Health Data Strategy: Expert Advisory Group. 2022. 3rd (final) report, May.
Public Policy Forum. 2022. Canadian Health Care’s Digital Future: Voices of Key Leaders, August.
Public Policy Forum. 2022. Next steps: Pan-Canadian Health Data Strategy, July.
Sanford. S., et al., 2022. The Impact of COVID-19 on Mental Health and Well-Being: A Focus on Racialized Communities in the GTA, Wellesley Insitute. March.
Trenaman, L., and J. Sutherland. 2020. Moving from Volume to Value with Hospital Funding Policies in Canada, Longwoods Healthcare Papers 19(2), May.
Tuohy, C.H. 2020. A new federal framework for long-term care in Canada, Policy Options. August.
Um, S-G. 2021. Leaving No One Behind in Long-Term Care: Enhancing Socio-Demographic Data Collection in Long-Term Care Settings, Wellesley Institute, July.
Wyonch, R. 2021. COVID Highlights Acute Shortage of Healthcare Workers, Commentary. Toronto: C.D. Howe Institute. February.
_________. 2021. Ounce of Prevention is Worth a Pound of Cure: Seniors’ Care After COVID-19. December.







