



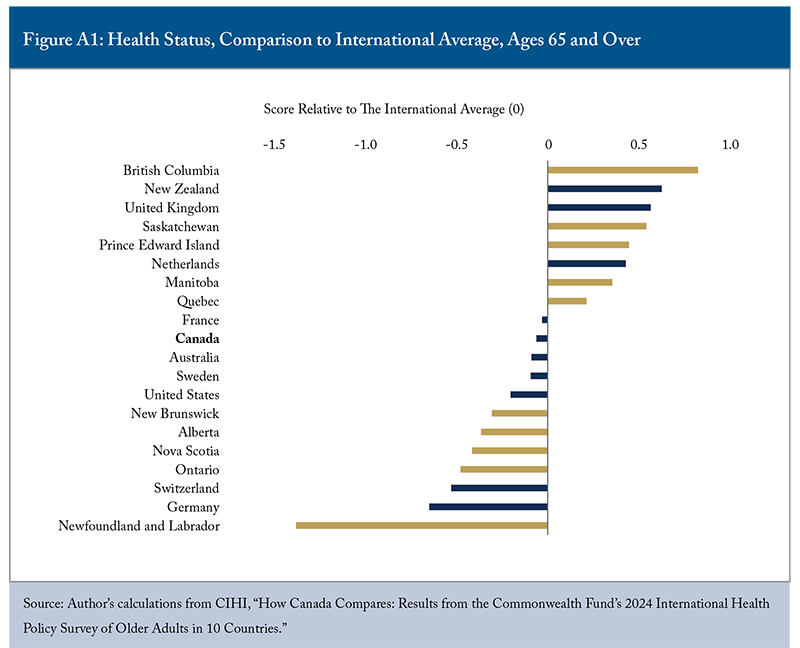
- Canada’s healthcare system ranks seventh for older adults among its international peers, ahead only of France, Germany, and Sweden. Canada performs above average in the care process and healthcare outcomes but ranks last in access to care, suggesting that while care delivery is often effective once patients enter the system, significant barriers remain at the point of entry.
- Most Canadian provinces fall significantly below the international average. Alberta and Ontario perform slightly above average, exceeding the performance of seven comparator countries. However, New Brunswick and Newfoundland and Labrador rank as the poorest performers, trailing all 10 comparator jurisdictions. Yet even high-performing Canadian provinces struggle with a critical weakness: timely access to care.
- The deteriorating state of timely access to care for seniors requires immediate attention. Closing remaining access gaps would allow PEI and Quebec to surpass the international average and BC to come close in overall healthcare performance. Canadian jurisdictions can learn from best practices in countries such as the Netherlands, which have successfully ensured access and after-hours care for their residents.
Introduction
Health systems worldwide face common pressures: ageing populations, funding constraints, workforce shortages, and rising inequalities. All grapple with the fundamental tension between controlling costs and improving patient outcomes. Yet some countries consistently outperform others through strategic resource allocation, innovative policy design, and effective adaptation to changing demands. These high-performing systems offer valuable lessons for strengthening Canada’s healthcare delivery.
More than half a million Canadians aged 65 and older lack a regular doctor or usual place of care – a growing and troubling concern. The 2024 Commonwealth Fund (CMWF) International Policy Survey of Older Adults11 The Commonwealth Fund survey involved adults aged 65 and older in Australia, Canada, France, Germany, the Netherlands, New Zealand, Sweden, Switzerland, the United Kingdom, and the United States. The survey respondents were asked about their interactions with healthcare systems and providers. Canada’s ranking relative to its CMWF peers is already reported in Gunja, Shah, and Leonard (2025). Their analysis covers 15 measures examining the performance of these 10 countries on access to care, coordination of care, and quality of care. ranked Canada last among 10 high-income countries for timely access to appointments and second-last for after-hours care. Canada also reports one of the highest rates of seniors visiting emergency departments (EDs) for non-urgent conditions. As the population ages and chronic disease prevalence rises, these access gaps will further strain EDs, raise system costs, and burden the broader economy. Monitoring both access to and quality of care for older adults is essential to maintaining their health and reducing pressures on the health system.
Benchmarking Canada’s healthcare systems against those of other high-income nations provides valuable insight into Canada’s relative performance and helps identify priorities for improvement. Provincial comparisons further illuminate which jurisdictions approach international standards and which lag significantly behind. This paper examines healthcare system performance across 10 high-income countries, including Canada, while assessing how individual provinces measure up internationally.
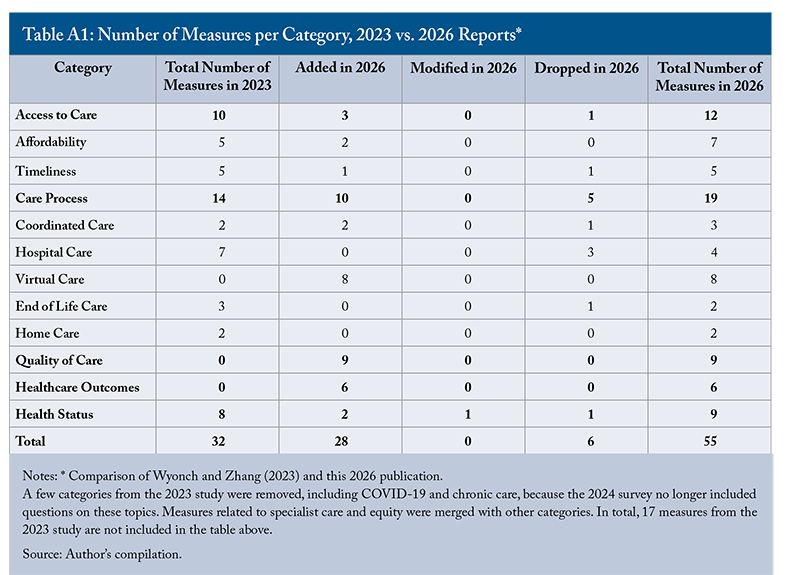
Similar to previous studies (e.g., Wyonch and Zhang 2023; Zhang 2025a), this paper analyzes performance across four categories: access to care, care process, quality of care, and healthcare outcomes. Most of these measures are derived from the 2024 CMWF survey provided by the Canadian Institute for Health Information (CIHI), with some statistics supplemented by the Organisation for Economic Co-operation and Development (OECD) and Public Health Agency of Canada.22 Of the 69 questions in the 2024 CMWF survey, 47 measures were selected for analysis. Most were selected and categorized according to the approach used by Wyonch and Zhang (2023). The changes in indicators between the 2023 report and this one are detailed in Appendix A. Full data and methodology details are in Appendix B. The results, therefore, reflect older adults’ reported experiences of access, affordability, and care delivery, which provide a valuable signal of system performance but do not capture all administrative or clinical dimensions of care.
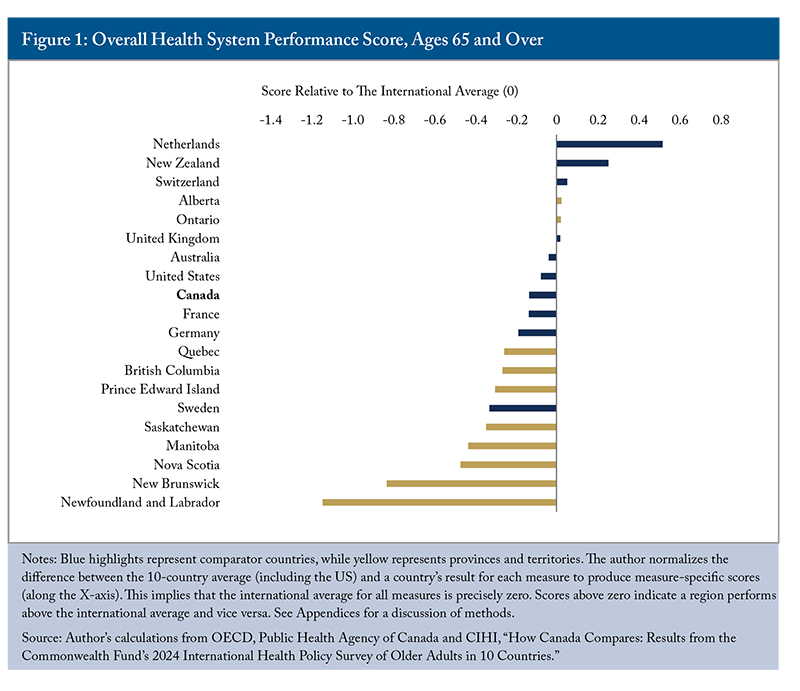
Most Canadian provinces fall significantly below the international average for overall healthcare performance for older adults, similar to the previous study (Wyonch and Zhang 2023). Alberta and Ontario perform slightly above average, exceeding the performance of seven comparator countries. However, New Brunswick and Newfoundland and Labrador rank as the poorest performers, trailing all 10 comparator jurisdictions.
Yet even high-performing Canadian provinces struggle with a critical weakness: timely access to care. Across all provinces, older Canadians face substantial barriers accessing same-day or next-day appointments and after-hours care, similar to the general population (Zhang 2025a). This consistent national deficiency stands in contrast to countries like the Netherlands and Germany, which excel at providing timely access through robust primary care infrastructure and extended service hours.
Improving access to care should be Canada’s top healthcare priority. Addressing this single dimension could elevate roughly half of provincial health systems to the international average. For struggling provinces like New Brunswick and Newfoundland and Labrador, the challenge is more comprehensive: they must simultaneously improve access, quality of care, and healthcare outcomes to approach the international average. This requires not just incremental adjustments but fundamental reforms to primary care delivery, payment models, and system accountability – lessons that high-performing countries have already implemented successfully.
Overall Health System Performance
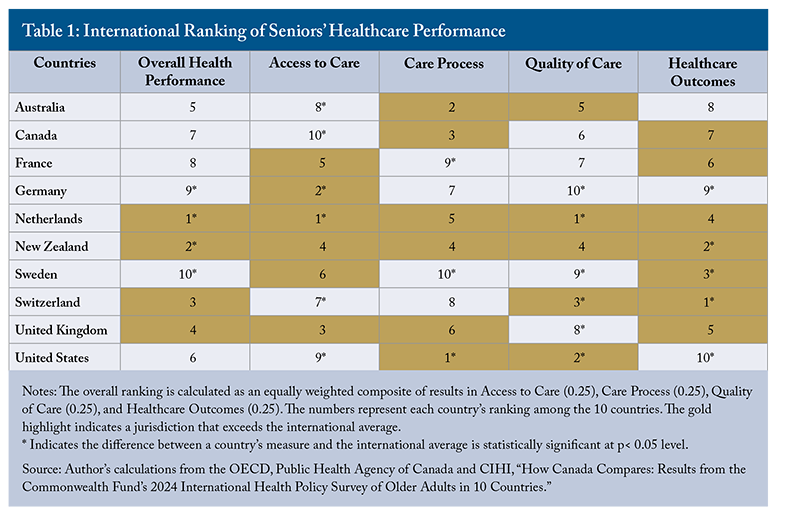
The top-performing countries in the 2024 survey were the Netherlands and New Zealand (Figure 1).33 While these comparisons are based largely on patient-reported experiences, they remain highly informative indicators of how effectively health systems deliver care to older adults in practice. New Zealand ranked fourth in access to care, care process and quality of care, and second in healthcare outcomes. It does not stand out as a top performer in a particular category, but has good results across the board, making it the second best overall. The Netherlands ranked first in both access to care and quality of care, and fourth in healthcare outcomes, demonstrating exceptional performance in affordability and accessibility. Its universal healthcare coverage creates minimal financial barriers, with only 0.6 percent of the general population reporting unmet medical needs (OECD 2025a). An impressive 99.5 percent of older adults have a regular doctor or place of care – the highest rate internationally – and the country reports the lowest difficulty accessing after-hours care, reflecting its robust primary care infrastructure. According to the OECD’s “Health at a Glance” report (2025a),44 The OECD’s “Health at a Glance” report mainly targets populations aged 15 and over. However, it still provides valuable insight for overall health system performance for seniors. 83 percent of Dutch residents were satisfied with their healthcare. These achievements stem from a system design that emphasizes patient and provider choice, regulated competition among insurers and providers, and cost-effective service delivery – all while maintaining high patient satisfaction (Blomqvist 2022; Wittevrongel, Eder and Faubert 2024). The Dutch model demonstrates that universal coverage, strong primary care, and market mechanisms can coexist successfully when properly structured and regulated.
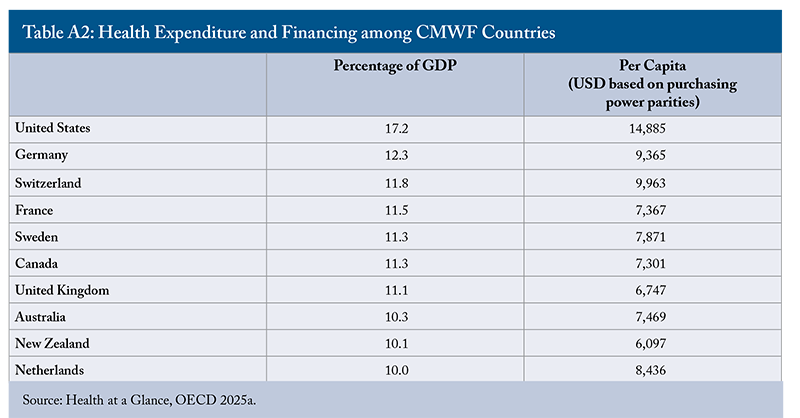
Canada ranked seventh overall despite spending a higher share of its GDP on healthcare than the Netherlands and New Zealand – 11 percent compared with 10 percent (Appendix C). Although Canada’s per capita health spending was lower than that of the Netherlands, it remained higher than New Zealand’s. This suggests that higher spending does not necessarily translate into better healthcare outcomes.
In 2024, OECD countries on average spent 9.3 percent of their GDP on health. The 10 countries in the CMWF survey all spent 10 to 12 percent of their GDP on healthcare. Canada’s health spending was 22 percent higher than the OECD average, but only 50 percent of the general population was satisfied with the availability of quality healthcare, well below the OECD average of 64 percent (OECD 2025a). Therefore, the issue is not insufficient funding but inefficient allocation and structural barriers that prevent resources from reaching frontline services effectively. According to the OECD (2025c), costs beyond fixed expenditures, such as salaries, inefficiencies and variations in medical practices, can lead to as much as 20 percent of health budgets being wasted without improving outcomes. Optimizing the use of existing healthcare resources is therefore critical.
Canada’s relative performance in seniors’ care is slightly better than its performance in total population healthcare, though it still ranks below the international average. Using survey responses from family physicians, the general population, and seniors, Zhang (2025a) ranked Canada 9th out of 10 countries, only ahead of the United States. Notably, the US is a poor performer overall, but it ranks first in the care process (Wyonch and Zhang 2023). This report shows a similar trend: the US ranks first in care process, but at or near the bottom of the rankings for access and healthcare outcomes.
Overall, Canada ranks among the top half of comparator countries in the care process category, but places last in access to care, sixth in quality of care, and seventh in healthcare outcomes (Table 1). In particular, it remains significantly below the international average on affordability and timeliness, as was the case for the general population (Zhang 2025a). The Netherlands and New Zealand are the only countries to rank above the international average in all categories. The Netherlands ranks first in access to care and quality of care, and Switzerland performs the best in healthcare outcomes.
Most provinces perform below the international average on overall healthcare performance for older adults (Figure 1). New Brunswick and Newfoundland and Labrador rank last among the comparator jurisdictions, with Newfoundland and Labrador scoring lowest in three of the four categories (Table 2). Prince Edward Island, Manitoba, and Saskatchewan also demonstrate substantial gaps, with deficiencies in most categories.
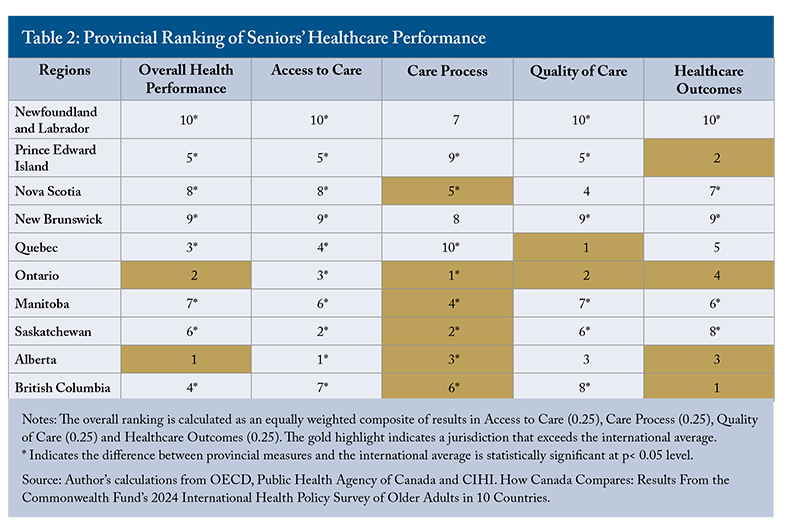
Alberta and Ontario stand out as the only provinces to exceed the international average, driven by strong care process performance and above-average healthcare outcomes. This pattern highlights a defining feature of Canada’s healthcare system: care delivery is often effective once patients are within the system, but significant barriers exist at the point of entry. All provinces – including Alberta and Ontario – struggle with access to care. This persistent access issue represents Canada’s most urgent healthcare challenge for older adults. That said, several provinces also require substantial improvements in care quality and healthcare outcomes to approach the international average.
Access to Care
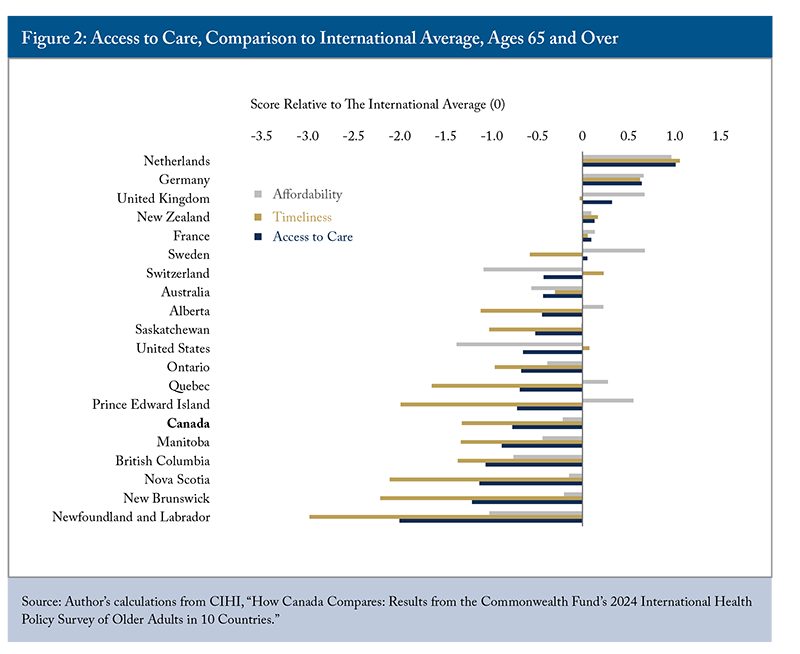
Access to care includes two subcategories: affordability and timeliness. Canada ranked last among its international peers in this category, worse than the general population’s results (Zhang 2025a). All provinces ranked below the comparator countries, except the United States (Figure 2), with New Brunswick and Newfoundland and Labrador ranking last.
Financial wellbeing is directly linked to access to healthcare, affecting people’s health status and potentially deepening poverty. Lower-income households and those with chronic conditions are particularly vulnerable. Most older adults across the 10 countries have some form of government and/or compulsory health insurance, but coverage for pharmaceuticals and dental care is often less comprehensive and differs in eligibility, premiums, copayments, and deductibles. As a result, out-of-pocket spending on health services, including prescription medications and dental care, varies widely by country. When these costs are unaffordable, older adults may delay or skip nonurgent care, leading to worsened health, delayed diagnoses, and higher overall system costs.
Affordability: Among the 10 countries, the United States and Switzerland55 Higher out-of-pocket spending in countries like Switzerland is likely linked to high-deductible health plans and to frequently needed services, such as dental and hearing care, that are not covered by the health insurance system (Gunja et al. 2024). performed the poorest in the affordability subcategory for older adults.
In 2024, over a quarter of older Canadians (25.8 percent) spent more than $1,000 out-of-pocket on medical treatments, a slight increase from the previous report (Wyonch and Zhang 2023). Manitoba stood out with the highest rate at 39.5 percent, far exceeding both the national and international averages. British Columbia and Newfoundland and Labrador reported the highest proportions of older adults forgoing medication due to cost, at approximately 10 percent each. In contrast, only 3 percent of older Quebecers reported this, below the CMWF average.66 Quebec has universal pharmacare coverage for prescriptions through government or employer insurance. Most provinces provide some publicly funded coverage for seniors and many of them have private insurance plans, but the variability of coverage and copayment rates across provinces is reflected in varying out-of-pocket costs. Quebec is the only province with mandated universal pharmacare coverage and its public insurance formularies generally cover more medications than other provinces. Although Canada’s proposed national pharmacare plan aims to improve access to essential prescription drugs, its slow rollout – with only three provinces and one territory signing bilateral agreements so far – has yet to make a measurable impact. Moreover, current coverage for seniors is limited to diabetes medications, leaving them to pay out-of-pocket for other prescriptions as well as for individuals without diabetes.
Oral health is vital to overall physical health, but many countries do not include dental care in their medical coverage. In Canada, only 6 percent of dental care was covered by public schemes, compared to 73 percent in Germany (OECD 2025a). While the majority of Canadians had private dental insurance in 2023-24 (61.6 percent), coverage was much lower among older adults.77 Health outcomes. Statistics Canada. https://www150.statcan.gc.ca/n1/pub/82-570-x/2024001/section2-eng.htm#a5_ As a result, more than one in five Canadian older adults (21.5 percent) skipped needed dental care due to cost, significantly higher than the international average of 13.6 percent,88 There are significant disparities in dental care affordability across jurisdictions: 15.9 percent of those surveyed in Saskatchewan responded that they skipped dental care or dental checkups due to cost, compared to 33.3 percent in Newfoundland and Labrador. with the highest rates again in Newfoundland and Labrador and British Columbia. By comparison, fewer than 5 percent of older adults reported skipping dental care in the Netherlands and Germany. In the Netherlands, dental care is not covered by national insurance, but provider rates are government-regulated (Gunja et al. 2024). In Germany, public insurance fully covers preventive care but only partly covers restorative dental care, prompting most residents to purchase supplemental dental coverage.
Since 2023, the federal government has launched the Canadian Dental Care Plan (CDCP) to reduce financial barriers to oral healthcare for uninsured, low- to mid-income Canadians (household net income below $90,000). The CDCP for seniors has rolled out in stages, with applications open for all seniors aged 65 and over as of May 2024, and full program access established by mid-2025.99 The 2024 CMWF survey, which was conducted between February 29 and June 20, 2024, does not reflect all changes made by the CDCP in terms of dental coverage for the population aged over 65. As of January 31, 2026, 6.27 million Canadians have been approved for coverage under the CDCP, and about 3.9 million have already received care.1010 Canadian Dental Care Plan statistics. https://www.canada.ca/en/services/benefits/dental/dental-care-plan/statistics.html According to Qureshi et al. (2026), the proportion of older Canadians who reported being unable to afford regular dental care decreased from 16 percent in 2024 to 11 percent in 2025, reflecting the early effects of the CDCP.
Overall, most provinces showed improvement across the same five affordability measures compared to 2021 (Wyonch and Zhang 2023), with New Brunswick, Alberta, and Quebec recording the greatest gains. PEI and Quebec were the only provinces with scores significantly above the international average in this subcategory.
Timeliness includes five indicators, such as having a regular doctor or place of care, same- or next-day appointments, and access to urgent after-hours care. Canada ranked last among 10 countries in this category, significantly below the international average, with three of the five measures at the bottom. All provinces scored far below the CMWF average, consistent with previous surveys (Zhang 2025a), with the Atlantic provinces performing worst. Compared to Wyonch and Zhang (2023), all provinces experienced decreases in the same four measures of timeliness. This confirms Canada’s persistent struggle to ensure timely access to care for its older population.1111 The difference from the international average is statistically significant for all provinces.
Having a regular doctor or place of care is essential for preventive care, early disease detection, and chronic disease management. Patients with a usual source of care are more likely to receive immunizations against flu, pneumonia, and respiratory syncytial virus, as well as blood pressure and cancer screenings (Gunja, Shah, and Leonard 2025). Continuity of care also fosters greater trust in the health system, encouraging patient engagement and better coordination. Canada ranked lowest on this measure, with 8 percent of older adults – approximately 600,000 – without a regular doctor or place of care, compared with the international average of 2.5 percent.1212 This indicator has steadily worsened over time: only 2 percent of older Canadians reported having no regular doctor or place of care in 2017, increasing to 4 percent in 2021 and 8 percent in 2024. Those living in rural areas, with lower incomes, or with fewer known medical needs are more likely to lack a primary care provider (CIHI 2025). Among the surveyed older adults, 33 percent reported having at least three chronic conditions, and 44 percent were taking four or more prescription medications, suggesting that inadequate primary care access could hinder their chronic disease management.
However, having a regular doctor or place of care is only the first step toward reliable access to care – care must also be available in a timely manner and outside regular hours, including evenings, weekends, and holidays (Gunja, Shah, and Leonard 2025). Across 10 surveyed countries, about a third of people reported waiting more than a week to see a doctor or nurse, with the longest waits in Canada, New Zealand and Sweden. In Canada, just a quarter of older adults were able to secure an appointment within 48 hours, significantly below the CMWF average of 39 percent. According to OECD (2025a), 9.1 percent of the Canadian population reported unmet medical needs (mainly due to waiting times), more than double the OECD average of 3.4 percent.
Among those needing after-hours care, more Canadians (71 percent) reported difficulties accessing it than their international peers (CMWF average: 59 percent). The challenge is most acute in the Atlantic provinces, where 74 to 88 percent of older adults struggled to obtain after-hours care. As a result, they were significantly more likely to use EDs for a condition that primary care practices could treat. This indicates inappropriate and inefficient healthcare. In the Netherlands, only 23 percent of older adults faced similar challenges. Its general practitioners can provide acute care out-of-office hours through a system of cooperatives (OECD 2025a). Expanding after-hours access is crucial, especially for seniors who face scheduling constraints, depend on working caregivers for transportation or support, or have family members balancing employment and caregiving responsibilities. Better access to after-hours care can also reduce reliance on EDs for non-urgent issues, freeing hospital capacity and saving money.
Since 2023, provinces across Canada have been implementing various initiatives to improve access (Zhang 2024). The increasing proportion of older Canadians unable to access necessary healthcare suggests that additional funding and new initiatives have yet to translate into widespread improvements in their access. Improving access to healthcare in Canada will require targeted investments and strategic efforts to ensure that those in need can access timely and appropriate services.
Care Process
Care process is a composite measure covering coordinated care, hospital care, virtual care, home care, end-of-life care (Table 3). The United States ranked first in this category, driven by strong performance across most subcategories, followed by Australia. Canada ranked ninth overall (among 20 jurisdictions), with most provinces performing above the international average, except Newfoundland and Labrador, Prince Edward Island, New Brunswick and Quebec. Common strengths across Canadian jurisdictions include coordinated and end-of-life care, where most provinces exceeded the international average. About half also performed above average in hospital, virtual and home care.
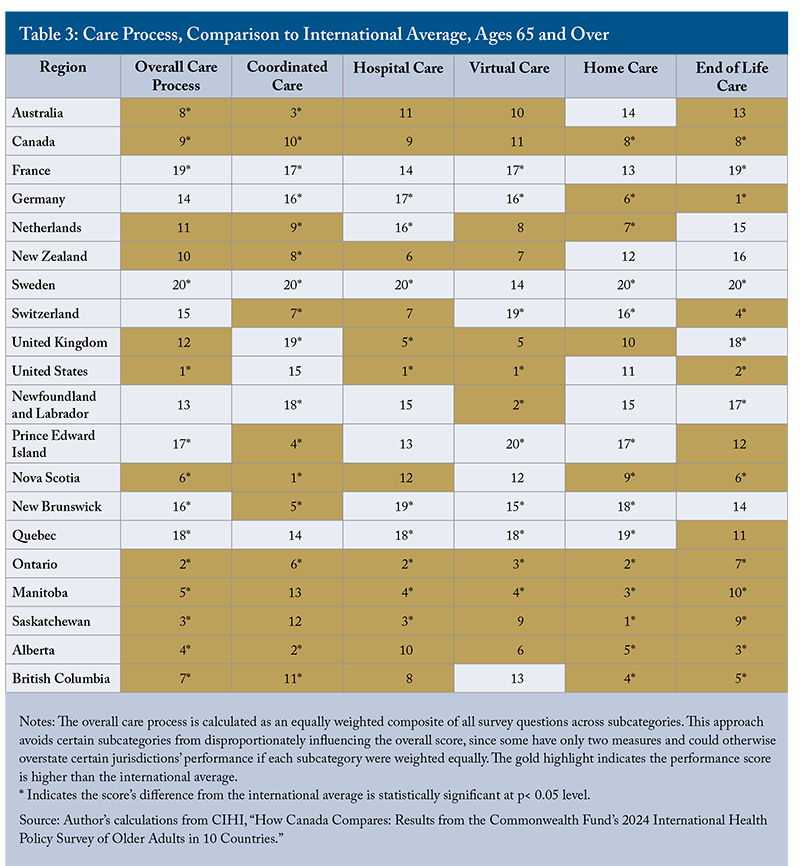
Coordinated Care includes communication between specialists and regular doctors and coordination between doctor visits. Canada ranked fifth among comparator countries, with most provinces scoring significantly above the international average.1313 Although Canada performed well in this subcategory, its performance has declined: in 2017, 82 percent of older adults reported that their primary care provider helped coordinate care with other doctors, dropping to 74 percent in 2021 and 66 percent in 2024. Similarly, the CMWF average decreased from 77 percent in 2017 to 59 percent in 2024. However, Newfoundland and Labrador performed significantly below the national average, particularly due to reports of poor communication between specialists and primary care physicians.
Hospital Care includes reviewing prescriptions, providing written instructions, arranging follow-up care, and providing services to help patients manage their health at home. Smooth transitions from hospital to home are critical for reducing complications and unnecessary readmissions (Gunja et al. 2024). The United States ranked highest in this subcategory, while older adults in Germany and Sweden reported the least coordinated care. Canada ranked fifth among comparator countries, with Ontario, Manitoba and Saskatchewan performing well above the international average, whereas New Brunswick and Quebec scored significantly below the national average. A lack of recommended care and treatment plans is frequently reported in these two provinces, which may lead to hospital readmissions or ED visits.
Virtual Care includes eight survey items assessing the use of virtual consultations, patient satisfaction with these visits and digital access to health information. The United States ranked first in this subcategory while Canada placed sixth. Some provinces, such as Newfoundland and Labrador, Ontario and Manitoba, scored significantly above the international average; however, PEI, New Brunswick and Quebec lagged furthest behind.
Online access to health information remains limited in Canada: only one in four older adults (27 percent) could view their test results online, compared with more than half in the United States. Similarly, the 2024 Canadian Digital Health Survey found that only 47 percent of Canadians have accessed personal health information online, despite 89 percent of respondents expressing interest in accessing it electronically.1414 Access to Electronic PHI. Canada Health Infoway. https://insights.infoway-inforoute.ca/2024-access-to-electronic-phi/ While digital technology has the potential to enhance care and patient experiences, older and less educated individuals may face challenges in understanding or navigating online systems (OECD 2025b). According to Jaana, Tamim, and Paré (2025), older Canadians make limited use of the internet to connect with healthcare professionals, access test results or patient portals, or book medical appointments. They find that groups most at risk of digital exclusion include rural residents, institutionalized older adults, and individuals with limited financial means or insurance coverage. Addressing these gaps requires targeted policy responses tailored to local and cultural environments. As electronic health record access expands across provinces,1515 For example, Nova Scotia and Newfoundland and Labrador have launched province-wide health portals, and New Brunswick has introduced the MyHealthNB app, which allows patients to view and share their patient summaries. targeted education initiatives will be crucial to help older adults use these tools effectively. Simplifying user interfaces, providing multilingual resources, and integrating voice-assisted technologies could enhance accessibility and digital inclusion.
Home care includes both services provided by health professionals and unpaid care received at home.1616 Notably, most jurisdictions reported lower percentages on these measures than in the 2021 survey. These declines align with patterns observed across the 10 surveyed countries. For example, in 2021, on average, 35 percent of older adults reported receiving home care from health professionals and 72 percent from unpaid caregivers, compared to 14 percent and 24 percent in 2024. This change may reflect reduced home care utilization following the COVID-19 pandemic, shifts in service delivery models, and other factors. Unlike the previous report (Wyonch and Zhang 2023), Canada ranked near the top internationally in this subcategory. However, PEI, New Brunswick and Quebec scored significantly below the international average, and their performance has worsened compared to 2021. In contrast, the remaining provinces have improved their relative international standing compared to 2021.
On average, about 17 percent of older adults across the 10 countries reported some difficulty with everyday activities, such as getting out of bed or using the toilet. In Canada, 16 percent said they received help from a professional compared to the CMWF average of 14 percent. Among those who received unpaid care, half preferred it, and 9.6 percent said the cost of professional services was too high. Provincial variations are significant: 25.9 percent of seniors in BC chose unpaid home care due to high costs, while no seniors in Ontario or Alberta indicated so.1717 The sample size is very small, so interpretation requires caution.
End-of-life care: Compared to their international peers, more older Canadians engage in end-of-life care planning: nearly two-thirds have discussed their care preferences for when they can no longer make decisions, and two-fifths have a written plan, both well above the international average. However, written plans do not guarantee that people ultimately receive the care they prefer.
The existing literature shows that most people would prefer to spend their final months or years at home, yet many families and patients cannot access sufficient medical, nursing, and social support during late-stage illness. Fewer than half of those who need end-of-life care actually receive it, indicating inadequate access (OECD, 2025a). As a result, hospitals remain the default setting for acute care and complex symptom management near death, driving substantial increases in health system costs in the final months of life (Quinn, Isenberg and Downar 2021).
In Canada, more than half of deaths occurred in hospitals, making them the most common place of death (OECD 2025a). The Netherlands is the only comparator country where home is the most common place of death, supported by its extensive home-based nursing and palliative care services, strong social infrastructure, and widespread palliative care training that prioritizes patient preferences. According to CIHI, half of Canadians died at home or in the community in 2023, with the lowest rate in Nova Scotia (42.1 percent) and the highest in Yukon (63.6 percent).1818 Death at Home or in Community. https://www.cihi.ca/en/indicators/death-at-home-or-in-community
In general, Canadian provinces perform well compared to international peers in the care process of older adults, with areas for improvement in specific provinces, such as Prince Edward Island, New Brunswick and Quebec.
Quality of Care
High-quality care requires health services to be safe, appropriate, clinically effective and responsive to patient needs (OECD 2025a). Indicators such as systematic medication reviews and avoidable hospital admissions reflect the safety and appropriateness of primary care, while 30-day mortality rates following acute myocardial infarction and stroke measure the clinical effectiveness of secondary care. In this category, the Netherlands ranked first, while Canada scored slightly below the international average (Figure 3). Most provinces recorded significant negative scores, with Newfoundland and Labrador performing worst; Quebec was the only province that scored significantly above the international average.
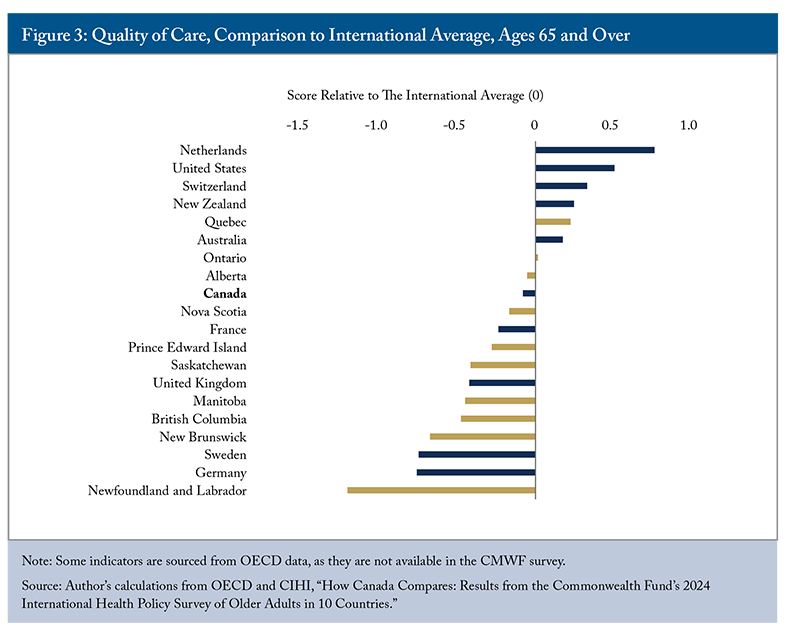
In Canada, 62 percent of older adults with a chronic condition discussed their main goals or priorities with a healthcare professional, similar to the CMWF average (CIHI 2025). Among those taking at least two prescriptions, three in four (76 percent) had their medications reviewed, well above the CMWF average of 69 percent. This suggests that older Canadians with chronic conditions receive relatively strong medication management support from primary care providers. Medication review remains important given that 42.3 percent of seniors in 2021-2022 were prescribed potentially inappropriate medications.1919 According to CIHI, this indicator is interpreted as the rate of seniors who take a medication identified as potentially inappropriate to prescribe to seniors because it is either ineffective or it poses unnecessarily high risk for older persons, and a safer alternative is available. https://www.cihi.ca/en/indicators/potentially-inappropriate-medication-prescribed-to-seniors This rate varies considerably across provinces, ranging from 32.4 percent in BC to 65.8 percent in New Brunswick.
While most older adults across 10 countries were satisfied with the quality of healthcare, only 73 percent of Canadians reported being satisfied – the lowest share among all countries. Provincial variation was significant, ranging from 59 percent in Newfoundland and Labrador to 77 percent in Ontario. About one in five older adults across countries said they were treated unfairly or felt their health concerns were not taken seriously. In Canada, higher rates were reported in Newfoundland and Labrador and New Brunswick. More than one-third of older Canadians reported unfair treatment due to age, followed by disability. Strengthening training to prevent ageism and ableism is essential to improving care experiences for older adults.
Healthcare Outcomes
Healthcare outcomes include measures such as life expectancy at 65, avoidable mortality, cancer deaths, and suicide rates. Switzerland and New Zealand performed best in this category, with Switzerland reporting the lowest avoidable mortality (114 deaths per 100,000 people) and New Zealand the lowest cancer mortality (109.5 deaths per 100,000; Figure 4).

Canada ranked seventh, slightly above the international average. Within Canada, British Columbia and PEI had strong outcomes, while the remaining Atlantic provinces, Manitoba and Saskatchewan scored significantly below average, mainly driven by higher cancer and suicide mortality.
For older adults, influenza vaccination is vital for reducing severe illness, hospitalizations, and seasonal strain on the healthcare system. All Canadian provinces reported higher flu immunization rates than the CMWF average. In particular, PEI, Nova Scotia and BC exceeded the World Health Organization’s 75 percent target, highlighting the success of their vaccination programs and efforts to ensure access and public trust.
Health Status
The overall health of older adults has implications for their quality of life and need to access healthcare. When seniors are generally healthy, systems can more easily deliver high-quality, accessible, and affordable care because demand pressures remain manageable. In 2024, 41 percent of older Canadians rated their health as very good or excellent, well above the CMWF average of 33 percent. Nearly three-quarters were taking two or more prescription medications, comparable to the international average.
However, the picture shifts once social determinants of health are considered.2020 Research shows that social drivers of health, such as socioeconomic, environmental, and behavioural factors, can account for up to half of health outcomes (Gunja et al. 2024). A higher share of older adults in several provinces reported being always or usually worried about basic needs such as food, housing costs, monthly bills, or income stability. In Newfoundland and Labrador, nearly 10 percent faced such financial concerns, roughly double the international average.
Overall, New Zealand, the United Kingdom, and the Netherlands performed best in this category, reflecting stronger social safety nets that reduce financial strain among older adults (Appendix D). Canada ranked slightly below average, with notable provincial variation. British Columbia, Saskatchewan, and PEI scored significantly above the international average, while the remaining Atlantic provinces, Ontario, and Alberta lagged behind.
Newfoundland and Labrador faced a particularly acute challenge: the poorest overall health status combined with the weakest informal support networks from friends, family, and community members. This dual vulnerability likely contributes to the province’s notably poor performance in care quality and healthcare outcomes, as seniors lacking informal assistance place greater demands on formal healthcare systems already struggling with capacity constraints.
Improvement Potential
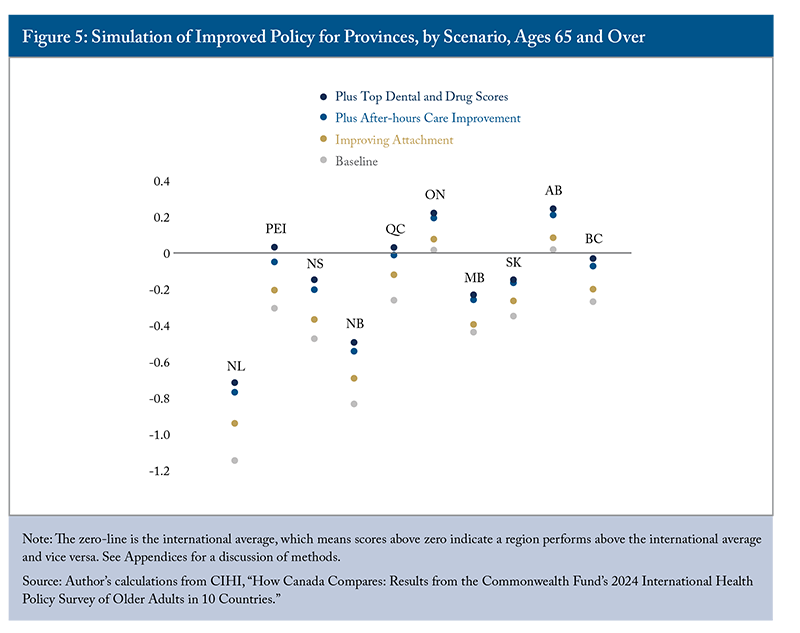
According to the 2024 CMWF survey, Canada’s seniors’ care has fallen behind that of its international peers, mainly in terms of access to care. To explore how Canadian provinces and territories could improve, I simulate scenarios in which these jurisdictions meet the highest international performance for specific survey indicators.
Scenario 1: Improving Attachment Only
Access to care requires both timely and affordable care. The first simulation focuses on improving attachment rates to match top performers like Germany and the Netherlands – all provinces would have 99 percent of older adults with a regular doctor or place of care. By doing so, most provinces would see a boost in access-to-care scores. Overall healthcare performance scores would also improve for most provinces; however, only Ontario and Alberta remain above the international average in the simulation (Figure 5). This implies that strong attachment to a primary care provider is only the first step toward addressing the access crisis.
While expanding the number of family physicians helps improve attachment, simply increasing physician supply alone is insufficient to meet the demands of a growing and ageing population.2121 For more information, see this Graphic Intelligence: https://cdhowe.org/publication/falling-behind-primary-care-access-deteriorates-as-population-outpaces-family-physician-supply/ Recent data show that Canada experienced a 1.9 percent increase in family physicians in 2024, the highest growth rate since 2019, yet the percentage of Canadians with a regular healthcare provider declined by 0.2 percent during 2023-24. All provinces except Ontario experienced declines, with PEI recording the sharpest decrease (Zhang 2025c).
As Zhang (2025a) argues, Canada already has a higher density of family physicians than comparator countries that achieve better population access outcomes. Quebec exemplified this paradox, as it has among Canada’s highest physician density yet suffers the worst primary care access (Zhang 2025d). Optimizing the efficiency and utilization of the existing workforce is, therefore, critical. Addressing current and future demands requires substantial reforms in the organization and funding of care delivery, along with an expanded scope of practice for other primary care providers (Zhang 2024). This requires reducing administrative burdens, implementing alternative payment models, and advancing team-based primary care, complemented by telehealth and remote monitoring to improve access while containing costs (Fierlbeck and Wyonch 2025).
Shehaed et al. (2023) find that countries with high rates of primary care attachment have stronger contractual agreements and accountability mechanisms for family physicians, including requirements regarding where they practise, their scope of practice, and patient acceptance criteria. In contrast, most family physicians in Canada operate as independent contractors with limited obligation or accountability to provincial and territorial health insurers. Countries such as the Netherlands mandate or strongly encourage patient registration with a general practitioner, offering an alternative model. These international examples offer valuable lessons for strengthening Canada’s primary care system (Zhang 2024).
Scenario 2: Improving After-hours Care Access
To improve patient care, provinces also need to increase appointment availability and flexibility. Suppose 51 percent of older Canadians can get appointments within 48 hours and only 37 percent experience difficulty obtaining after-hours care, like those in Germany and the Netherlands.2222 Improving attachment and improving after-hours care are treated as independent variables for illustration purposes. As a result, the effects of improved attachment on after-hours care are not included in the analysis, potentially underestimating its impact. However, given that 71 percent of older adults faced difficulty accessing after-hours care despite 92 percent having an established attachment, improving attachment alone may have minimal effects on after-hours care availability. In that case, all provinces will see further improvement in access to care, with five moving from negative to positive scores. More importantly, Quebec will see its overall health performance move from below to near the international average.
The Netherlands provides universal coverage while ensuring people can access care when needed. General practitioners (GPs) in the Netherlands are required to provide at least 50 hours of after-hours care annually to maintain their professional licensure. Most GPs also participate in cooperatives2323 After-hours primary care is provided by 119 large-scale primary care physician cooperatives, each of which has 50 to 250 physicians who provide care to 100,000 to 500,000 citizens (Smits et al. 2017). The cooperatives serve 99 percent of the Dutch population of 17 million and are available daily from 5 p.m. to 8 a.m. on weekdays and all hours on weekends. that offer care during evenings and weekends. These cooperatives collaborate with and are often located within hospital emergency departments to reduce unnecessary ED visits (Smits et al. 2017). Primary care physicians in these cooperatives are responsible for triaging and treating walk-in patients who would otherwise go to EDs after hours. More than half of the cooperatives are fully integrated with hospital emergency departments, forming what are known as “emergency care access points.” The reorganization has led to a 13 to 22 percent reduction in overall ED use, providing a safe and cost-effective alternative to traditional ED care (Smits et al. 2017). This model offers Canada valuable lessons for redesigning after-hours care.
In some provinces, such as Ontario and Quebec, physician contracts for team-based care include requirements for after-hours availability. However, there are currently no regulations enforcing these requirements, resulting in significant variation in care hours across regions and teams. Addressing this gap is essential to ensure that older adults across Canada have reliable access to care when they need it.
Scenario 3: Improving Drug and Dental Care Access
Reducing cost barriers to drug and dental care would also improve the overall health performance ranking of provinces. If Canadian provinces improved drug and dental access to levels with the top two performers (where only 2.6 percent of older adults skip medications and 4.4 percent forgo dental care), alongside improvements in attachment and after-hours care, Nova Scotia and New Brunswick would also have positive access-to-care scores. This improvement also moves PEI and Quebec above the international average for overall health performance, while bringing BC into parity with it. Moreover, Ontario and Alberta’s performance would be comparable to New Zealand’s.
All provinces have prescription drug coverage programs for seniors and low-income households, with different rules on premiums, copayments, and income levels. A catastrophic coverage analysis examined household spending burdens across income quintiles and demographic groups, revealing that lower-income households and seniors faced disproportionate pharmaceutical cost challenges (Wyonch 2025). Each province also has different drug formularies, meaning different gaps in access or pharmacare support exist.
Quebec offers critical lessons for other provinces, as it has the lowest percentage of seniors skipping prescription medications due to cost. This success stems from Quebec’s unique pharmacare model, which requires all seniors to enroll in either a public drug plan, a private insurance plan, or a combination of both if supplemental coverage is available. The public plan includes income-based premiums and copayments,2424 Annual premium ranges between $0 and $766 per person, depending on net family income. The monthly deductible is $22, with a 30 percent copayment, up to an annual maximum of $1,232. Seniors aged 65 or over who receive less than 94 percent of the maximum Guaranteed Income Supplement have a maximum copayment of $687 instead. For more information, see https://www.ramq.gouv.qc.ca/en/citizens/prescription-drug-insurance/rates-effect but seniors who receive 94 percent or more of the Guaranteed Income Supplement (GIS) benefit from full coverage with no premiums or copayments. Even in provinces such as Nova Scotia and New Brunswick, where premiums are waived for GIS recipients, copayments still create cost barriers for seniors who rely on multiple prescriptions or fall just short of eligibility for income assistance. (Seniors in New Brunswick and Newfoundland have the lowest median income in Canada).2525 Statistics Canada. Table 11-10-0239-01. Income of individuals by age group, sex and income source, Canada, provinces and selected census metropolitan areas. DOI: https://doi.org/10.25318/1110023901-eng Moreover, variations in copayment rates and maximum out-of-pocket charges across provinces disproportionately affect financially vulnerable seniors, highlighting the need for more equitable access to prescription medications.
Prince Edward Island stands out for its recent efforts, working with the federal government to lower deductibles, reduce copayments, broaden the provincial drug formulary and expand eligibility for public drug coverage.2626 According to its Senior Drug Program plan, seniors in PEI pay $8.25 plus $7.69 of the pharmacy professional fee for each eligible prescription they fill. Any remaining cost will be covered by the program. For more information, see https://www.princeedwardisland.ca/en/information/health-and-wellness/seniors-drug-program These reforms have improved residents’ access to prescriptions and offer a practical model for other jurisdictions. To ensure seniors with low income and multiple chronic conditions can access essential medications when needed, provinces across Canada need to strengthen their drug coverage programs.
Internationally, Germany’s health system offers a particularly instructive example. Public insurance covers 82 percent of pharmaceutical costs and 73 percent of dental care, with patient expenses capped at 2 percent of gross income and just 1 percent for those with chronic illness, providing strong protection against financial hardship. By contrast, in Canada, only 36 percent of pharmaceuticals and 6 percent of dental care costs were covered by public programs, leaving many Canadians, including seniors, to rely on private benefit plans or pay out of pocket for the full costs of care. This situation may improve as the CDCP expands access to basic dental coverage for seniors without existing insurance, and as more eligible seniors begin receiving care under the program.
Canadian provinces can draw valuable lessons from these domestic and international examples. By improving program design, minimizing out-of-pocket costs, and expanding drug formularies, governments can close existing gaps and move closer to universal coverage. With ongoing federal initiatives addressing pharmacare and dental care, these goals are achievable and will help ensure that all Canadian seniors, regardless of income or health status, can afford the care they need.
Conclusion
Benchmarking Canada’s healthcare system against international peers shows our relative performance and priority areas for improvement and provides international examples that can inform domestic policy and healthcare delivery changes.2727 See Appendix E for data limitations. The 2024 CMWF survey reveals systemic barriers, such as low attachment rates, limited appointment availability, and difficulties obtaining after-hours care, which continue to limit access to essential healthcare for older Canadians.
In international comparisons, Canada ranks seventh out of 10 countries, performing last in access to care. However, Canada performs very well in the care process category. Many Canadian provinces excel in coordinated care and end-of-life care. Nevertheless, most Canadian provinces fall significantly below the international average for overall healthcare performance. Alberta and Ontario perform slightly above the average, better than seven comparator countries. In contrast, New Brunswick and Newfoundland and Labrador are the poorest performers, ranking last among the comparator jurisdictions.
Older adults are, on average, the highest-cost users of our healthcare services, and as Canada faces an ageing population, addressing their needs is essential. The deteriorating state of timely access to care for seniors requires immediate attention. Canadian jurisdictions can learn from best practices in countries such as the Netherlands, which have successfully ensured access and after-hours care for their residents.
While most seniors have some drug and dental coverage, affordability gaps exist, especially for those with complex conditions and lower incomes. Improving program design, reducing out-of-pocket costs, and expanding drug formularies will help close these gaps. Targeted interventions would be more effective, as cost-related challenges for prescription drugs and dental care are concentrated in certain sociodemographic groups and provinces. For example, older adults in Newfoundland and Labrador and British Columbia reported the greatest financial barriers. Focusing resources where affordability barriers are greatest will deliver the strongest return on investment. Recent expansions in drug and dental care coverage, although not yet captured in the latest survey, may improve Canada’s performance in the affordability subcategory.
Closing remaining coverage gaps and enhancing timely access to care would allow PEI and Quebec to surpass the international average and BC to come close in overall healthcare performance. The remaining provinces, including New Brunswick and Newfoundland and Labrador, will also need to strengthen other areas, such as care quality and healthcare outcomes, to move closer to the international average.
Strengthening primary care is an effective way to improve health outcomes and reduce wasteful spending by limiting unnecessary hospitalizations and emergency department visits. Given competing policy priorities and current public finance constraints, significant new health spending is unlikely. Evidence from top-performing countries shows that it is possible to spend wisely by emphasizing value-based care. Targeted investments that enhance both access and quality can yield better outcomes without driving up overall costs. Placing greater emphasis on health outcomes and containing costs through improved efficiency and effectiveness represents a viable path forward to ensure the healthcare system meets the needs of all older adults across Canada.
Appendix A:
The analysis relies on data collected from the 2024 CMWF international survey. Of 69 questions, 47 were selected for analysis. Most of the measures were selected and categorized based on those presented in Wyonch and Zhang (2023). Measures that did not fit within these categories were excluded. However, several new measures were added as the 2024 CMWF survey expanded to include additional information, such as virtual care, providing valuable insights to complement the existing categories. The Commonwealth Fund provides a range of useful, reasonable healthcare performance indicators, but it is not comprehensive. To address this, the author incorporated additional data points from the OECD and Public Health Agency of Canada. The table below compares the number of measures for each category between the 2023 C.D. Howe Institute report and the current analysis.
Appendix B:
Data
The Commonwealth Fund’s 2024 International Health Policy Survey of Older Adults randomly sampled the population age 65 and older in 10 countries: Australia, Canada, France, Germany, the Netherlands, New Zealand, Sweden, Switzerland, the United Kingdom and the United States. The Canadian survey was conducted between February 29 and June 20, 2024.
The Commonwealth Fund funded 750 completed interviews across Canada. The Canadian Institute for Health Information funded additional interviews to complete at least 250 in each province. Funding was also provided to increase sample sizes in Quebec (Commissaire à la santé et au bien-être, ministère de la Santé et des Services sociaux du Québec) and in Ontario (Ontario Health). In total, 3,989 interviews were conducted across Canada, including 1,014 in Quebec and 946 in Ontario.
Data were weighted to ensure the final outcome was representative of the adult population aged 65 and older in each country. Weighting procedures considered sample design, probability of selection, and systematic nonresponse across known geographic and demographic parameters, including region, sex, age, education, and other characteristics relevant to the population of each country.
Methodology
Similar to previous publications (Busby, Muthukumaran, and Jacobs 2018; Wyonch and Zhang 2023; Zhang 2025a), the author converted each country’s results (e.g., the percentage of survey respondents giving a particular response) into a normalized performance score. This score was calculated as the difference between the country’s results and the 10-country mean, divided by the standard deviation of the results for each measure. This implies that the international average for all measures is precisely zero. A positive performance score indicates the country performs above the 10-country average; a negative score indicates the country performs below the international average. The overall ranking is calculated as an equally weighted composite of results across the categories of Access to Care (0.25), Care Process (0.25), Quality of Care (0.25), and Healthcare Outcomes (0.25). Sensitivity analysis shows that applying different weights to these categories changes the rankings of middle countries, but the rankings of the top and bottom countries remain the same. That is, the Netherlands and New Zealand remain top-performing countries, while France and Sweden are the bottom-performing.
Appendix C:
Appendix D:
Appendix E:
Data Limitations
Countries with high-performing primary care, such as the UK and New Zealand, often survey their patients about the system. However, in Canada, the standardized cross-provincial data, let alone cross-national data, on health system performance are limited. The CMWF survey offers unique and detailed data on patients’ experiences; however, it does not capture administrative or financial information that would enable more direct comparative analysis of policies. The Commonwealth Fund survey cannot draw conclusions about the relative efficiency or resulting clinical outcomes of specific policies in other jurisdictions. Notably, some experts caution about the limits of ranking exercises because they do not specifically account for each province’s distinct demographic and socioeconomic circumstances (Hewitt and Wolfson 2013). The author is aware of the potential bias related to survey data. Possible data limitations include sampling bias, response bias, and cross-cultural variations. However, the findings still add value and provide a broad, comparable overview of older adults’ perceptions and interactions with healthcare systems and providers. It can highlight priority areas for improvement and allow for comparison across many aspects of care. Cross-province results also could facilitate the identification of best practices, thereby enabling more targeted engagement from pan-Canadian health organizations. Moreover, international comparisons would inform the Canadian public about healthcare performance relative to top international performers, fostering a political environment receptive to further reform.
The author extends gratitude to Don Drummond, Nicholas Dahir, Parisa Mahboubi, Samir Sinha, Rosalie Wyonch, Jennifer Zelmer, and several anonymous referees for valuable comments and suggestions. The author retains responsibility for any errors and the views expressed.
REFERENCES
Canadian Institute for Health Information. 2025. “Survey Shows How Healthcare Experiences of Older Adults in Canada Compare Internationally.” https://www.cihi.ca/en/survey-shows-how-health-care-experiences-of-older-adults-in-canada-compare-internationally
Gunja, Munira Z., Gretchen Jacobson, Faith Leonard, and Reginald D. Williams II. 2024. “Health Care Affordability for Older Adults: How the U.S. Compares to Other Countries.” Commonwealth Fund. December. https://doi.org/10.26099/tgjb-1m67
Gunja, Munira Z., Arnav Shah, and Faith Leonard. 2025. “Access and Quality of Care for Older Adults in 10 Countries: Findings from the 2024 Commonwealth Fund International Health Policy Survey of Older Adults.” Commonwealth Fund. April. https://doi.org/10.26099/4wrj-kj97
Jaana, Mirou, Haitham Tamim, and Guy Paré. 2025. “eHealth and the Digital Divide Among Older Canadians: Insights from a National Cross-Sectional Study.” Journal of Medical Internet Research 27: e72274. doi:10.2196/72274.
OECD. 2025a. “Health at a Glance 2025: OECD Indicators.” OECD Publishing, Paris. November. https://doi.org/10.1787/8f9e3f98-en.
____. 2025b. “Does Healthcare Deliver? Results from the Patient-Reported Indicator Surveys (PaRIS): Canada.” OECD Publishing, Paris. https://www.oecd.org/en/publications/2025/02/does-healthcare-deliver-results-from-the-patient-reported-indicator-surveys-paris-country-notes_40213115/canada_1c5b9091.html
____. 2025c. “Health as an Economic Imperative Synthesis Report.” OECD Publishing, Paris. https://www.businessatoecd.org/hubfs/Policy%20Groups/20.%20Health/FIN-2025-03%20Health%20as%20an%20Economic%20Imperative%20-%20Business%20at%20OECD%20(BIAC)%20Health%20Forum%202024%20Synthesis%20report.pdf
Quinn, Kieran, Sarina Isenberg and James Downar. 2021. Expensive Endings: Reining In the High Cost of End-of-Life Care in Canada. Commentary 608. Toronto: C.D. Howe Institute. https://cdhowe.org/publication/expensive-endings-reining-high-cost-end-life-care-canada/
Qureshi, Tazeen, Gabrielle Gallant, Talia Bronstein, Mark Hazelden, Alyssa Brierley and Samir Sinha. “Perspectives on Growing Older in Canada: The 2025 NIA Ageing in Canada Survey.” Toronto, ON: National Institute on Ageing (2026), Toronto Metropolitan University.
Shahaed, Heba, Richard H. Glazier, Michael Anderson, Erica Barbazza, Véronique L.L.C. Bos, Ingrid S. Saunes, Juha Auvinen, Maryam Daneshvarfard, and Tara Kiran. 2023. “Primary care for all: lessons for Canada from peer countries with high primary care attachment.” Canadian Medical Association Journal 195(47): E1628-E1636. Available at https://doi.org/10.1503/cmaj.221824
Smits, Marleen, Martijn Rutten, Ellen Keizer, Michel Wensing, Gert Westert, and Paul Giesen. 2017. “The Development and Performance of After-Hours Primary Care in the Netherlands: A Narrative Review.” Annals of Internal Medicine 166(10):737-742. May 16. https://doi.org/10.7326/m16-2776
Wyonch, Rosalie, and Tingting Zhang. 2023. “Shortcomings in Seniors’ Care: How Canada Compares to its Peers and the Paths to Improvement.” E-Brief. Toronto: C.D. Howe Institute. https://cdhowe.org/publication/shortcomings-seniors-care-how-canada-compares-its-peers-and-paths/#shortcomings-in-seniors--care--how-canada-compares-to-its-peers-and-the-paths-to-improvement
Wyonch, Rosalie. 2025. “Access and Affordability: Building Fiscally Responsible Pharmacare Systems.” Toronto: C.D. Howe Institute. https://cdhowe.org/publication/access-and-affordability-building-fiscally-responsible-pharmacare-systems/
Fierlbeck, Katherine, and Rosalie Wyonch. 2025. Disconnected: Inside Canada’s Patchwork of Virtual Care. Commentary 701. Toronto: C.D. Howe Institute. https://cdhowe.org/publication/disconnected-inside-canadas-patchwork-of-virtual-care/
Zhang, Tingting. 2024. The Doctor Dilemma: Improving Primary Care Access in Canada. Commentary 660. Toronto: C.D. Howe Institute. https://cdhowe.org/publication/doctor-dilemma-improving-primary-care-access-canada/
__________. 2025a. Troubling Diagnosis: Comparing Canada’s Healthcare with International Peers. Commentary 673. Toronto: C.D. Howe Institute. https://cdhowe.org/publication/troubling-diagnosis-comparing-canadas-healthcare-with-international-peers/
____________. 2025b. “Canada’s Electronic Health Record Gap: Patients Deserve Better.” Intelligence Memo. Toronto: C.D. Howe Institute. June 6. https://cdhowe.org/publication/canadas-electronic-health-record-gap-patients-deserve-better/
___________. 2025c. “Federal Health Funding: Promises and Performance Gaps.” Intelligence Memo. Toronto: C.D. Howe Institute. November 6. https://cdhowe.org/publication/federal-health-funding-promises-and-performance-gaps/
___________. 2025d. The Quebec Primary Care Conundrum: Good Intentions, Persistent Problems. Commentary 700. Toronto: C.D. Howe Institute. https://cdhowe.org/publication/the-quebec-primary-care-conundrum-good-intentions-persistent-problems/